
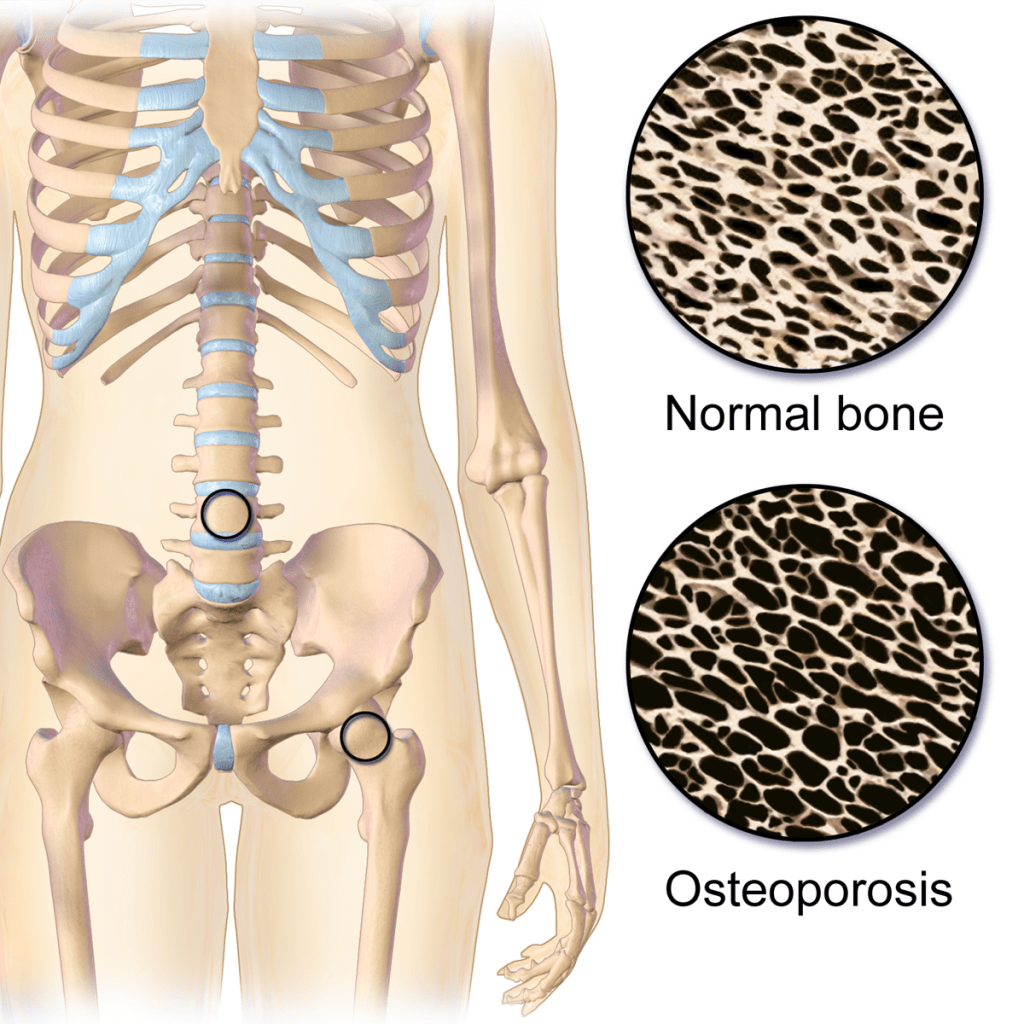
Osteoporosis is a condition in which bones lose strength, becoming more likely to break and producing changes in posture. It is especially common in women after the menopause, in older adults, in people with a family history of fractures, in those who are underweight, smoke, drink heavily, use steroid medicines for a long time, get little exercise, or have health problems that reduce nutrient absorption or affect hormones. The main danger is fracture, especially of the hip, spine, and wrist, and these breaks can cause pain, loss of independence, deformity, and a long recovery.

Conventional treatment
The main goal of treatment is to prevent fractures. That means not only medicine, but also enough calcium and vitamin D, regular weight-bearing and strength exercise, fall prevention, stopping smoking, limiting alcohol, and treating any underlying cause such as thyroid problems or malabsorption.
The most common medicines are bisphosphonates, such as alendronate, risedronate, and zoledronic acid. These slow bone loss and are well proven to lower the risk of spine, hip, and other fractures. The main drawbacks are stomach or esophagus irritation, muscle or joint aches, and, rarely, more serious problems like unusual thigh fractures or jaw bone damage.
Denosumab is another effective drug that also reduces fracture risk by slowing bone loss. It is usually given as a subcutaneous injection every 6 months for osteoporosis. It is often used when bisphosphonates are not suitable. It can cause low calcium, skin infections, and rare jaw or thigh problems. One important caution is that it should not be stopped suddenly without a plan, because bone loss can rebound quickly.
For people at very high risk, doctors may use bone-building medicines such as teriparatide, abaloparatide, or romosozumab. These are usually reserved for more severe osteoporosis because they are stronger, more specialized treatments and can have their own side effects.
Some women may be offered raloxifene, which is a SERM, or selective estrogen receptor modulator. In simple terms, it acts like estrogen in some places, such as bone, and blocks it in others. It can help protect the spine, but it may cause hot flashes and increase the risk of blood clots.
For women around and after menopause, hormone replacement therapy (HRT) can help protect bone because estrogen helps slow bone loss. It is most often considered when a woman also has bothersome menopausal symptoms such as hot flushes, night sweats, or vaginal dryness, so the bone benefit can be part of a broader treatment plan rather than the only reason to use it.
That said, HRT is not a one-size-fits-all answer. It can be very helpful for some women, but it also has important risks and is not suitable for everyone. The main concerns depend on the type of HRT, age, time since menopause, and personal history, but may include blood clots, stroke, breast cancer risk in some settings, and other hormone-related issues. So the decision is usually individualized: if a woman is a good candidate and has menopausal symptoms plus bone loss risk, HRT can be a sensible option; if not, other osteoporosis treatments may be safer or more appropriate.
Balancing risks and benefits
It is completely reasonable to worry about rare but serious side effects. No one wants to trade one problem for another. But the real question is not whether a medicine has risks — almost all medicines do — but whether the risks are smaller than the harm that is likely to happen without treatment.
That comparison matters because osteoporosis itself can cause major damage. A hip fracture, for example, can lead to surgery, loss of mobility, chronic pain, and permanent loss of independence. A spine fracture can also be painful and can gradually change posture and breathing. For many people with clearly high fracture risk, the chance of preventing one of these events is much more important than the small chance of a rare medication complication.
The best approach is to match the treatment to the person. Someone with mild bone loss may not need aggressive therapy. Someone with a prior fragility fracture, very low bone density, or multiple risk factors may benefit a great deal from medication. It also helps to review dental health, kidney function, past medication use, and how long treatment should continue, because those details can lower risk further. So the sensible attitude is not “medicines are dangerous” or “medicines are harmless,” but “use the least risky effective option for the situation.”
When talking about HRT (or any medicine), it is important to understand the difference between percentage risk increase and absolute risk increase. A percentage increase tells you how much the risk changes compared with the starting point, but it does not tell you how common the problem is in the first place. For example, if a rare problem doubles from 1 case in 10,000 women to 2 cases in 10,000 women, that is a 100% increase in percentage terms (sounds alarming!), but the actual increase is only 1 extra case per 10,000 women (not so alarming!).
That is why the absolute number matters so much. Some forms of HRT, especially tablets taken by mouth, can slightly raise the risk of blood clots and breast cancer, but the real increase is still small in many women. Patches and gels appear to carry less clot risk than tablets. So the best way to think about HRT is not just “Is there a risk?” but “How big is the risk in real life, and does it outweigh the benefits for this person?”
Combined HRT can slightly increase the risk of blood clots and breast cancer, but the absolute increase is small. For example, one large UK study found about 9 extra blood clots per 10,000 women per year with HRT tablets, while patches and gels did not increase clot risk. For breast cancer, the NHS estimates about 5 extra cases per 1,000 women over 5 years with combined HRT. These figures help readers see the real size of the risk instead of just hearing a percentage increase.
Supplements
The most useful supplements are calcium and vitamin D, especially when intake is low or deficiency is present. Vitamin D helps the body absorb calcium, and calcium provides the raw material for bone.
It has to be said that the evidence for supplements is underwhelming, with the best evidence being for calcium and vitamin D, but even here the quality of evidence for either when used alone is quite low. It is better when they are used together:
| Option | Evidence for preventing loss of bone | Evidence for preventing fractures |
|---|---|---|
| Calcium + vitamin D | Moderate | Moderate |
| Vitamin D alone | Low to moderate | Low |
| Calcium alone | Low | Low |
Thus, these have to be regarded as supportive measures, not a replacement for osteoporosis medicines when fracture risk is high.
There are some other minerals with scientifically plausible but unproven actions in preventing bone loss, notably magnesium, zinc and boron. Their significance is greater if there is a demonstrated or likely deficiency.
Magnesium is important for bone health too. Low magnesium can happen with poor diet, diarrhea, malabsorption, alcohol use, diabetes, or certain medicines. It is not a stand-alone osteoporosis treatment, but correcting a deficiency can be worthwhile.
Zinc also matters because it helps with bone formation and repair. Deficiency is more likely when diet is poor, absorption is reduced, or the body’s needs are increased. Again, the goal is usually to correct a deficiency rather than use zinc as a main osteoporosis treatment.
Boron has some interesting biological roles in bone and mineral metabolism, but the evidence is still limited. It is better viewed as a minor supporting nutrient than a core part of osteoporosis care.
Herbs
Herbs are the least proven part of the picture. They may have a supportive role, but they should not be treated as substitutes for proven treatment.
In Traditional Chinese Medicine, the best-known studied formula is ELP, made from Epimedii Herba, Ligustri Lucidi Fructus, and Psoraleae Fructus. It has some encouraging research behind it, but the evidence is still much weaker than for standard osteoporosis medicines. Other TCM herbs have also been studied, but most of the evidence is preliminary.
In Western herbal medicine, herbs such as nettle leaf, oat straw, horsetail, and red clover are sometimes discussed for bone support. They are usually used as nourishing or menopausal-support herbs rather than as direct osteoporosis treatments. Their evidence is limited, and some may have safety or interaction concerns.
Practical take
The most useful way to think about osteoporosis is this: the main goal is to prevent broken bones. For many people, that starts with healthy habits, enough calcium and vitamin D, and regular weight-bearing exercise. If the risk of fracture is higher, a doctor may also recommend a medicine that can make bones stronger. Supplements and herbs may help in some cases, but they are usually extras rather than the main treatment.
Images:
- Blausen.com staff (2014). «Medical gallery of Blausen Medical 2014». WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436., CC BY 3.0 https://creativecommons.org/licenses/by/3.0, via Wikimedia Commons.
- BruceBlaus, CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons.
